
Table of Contents
Abstract
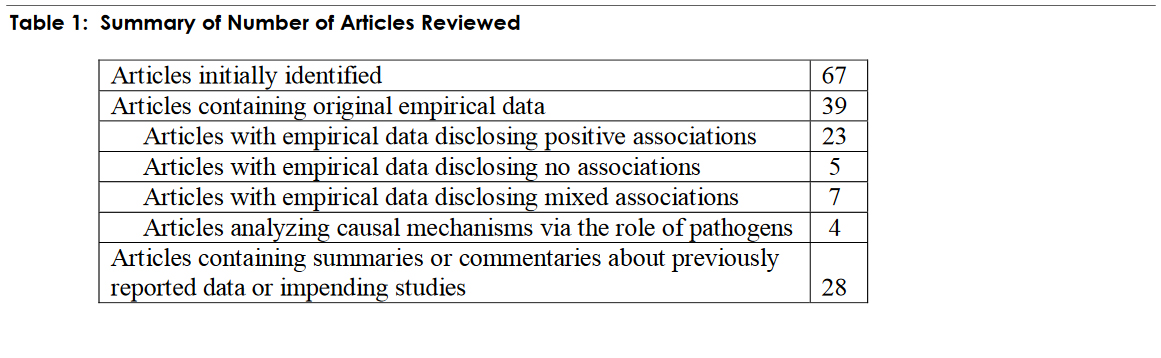
During the last decade numerous investigators have studied the posited relationship between periodontal disease in pregnant women and adverse pregnancy outcomes such as premature labor, pre-term deliveries, small-for-gestational age infants, early or late miscarriages, low birth weights and pre-eclampsia. This article presents the results of a comprehensive literature review of these investigations as well as other articles containing similar summaries or commentaries about the studies. The review objective was to ascertain and summarize what the investigators have concluded about this topic. Articles were obtained from the authors’ files, references provided in other publications, articles shared by colleagues, and articles listed in PubMed©, many of which were obtained through interlibrary loans at the University of Utah, Salt Lake City, Utah. The authors identified 67 initial articles. Of those 67, 39 contained original empirical data. Twenty-three of the 39 disclosed positive associations, 5 disclosed no associations, 7 revealed mixed associations (both positive and no associations depending on the variables analyzed). Another 4 articles analyzed, in a preliminary sense, the role of pathogens as potential causal explanations for positive associations. The remaining articles contained summaries or commentaries about previously reported data or impending studies. Despite all of the research that has occurred, clearly there still isn’t sufficient evidence to conclude or explain definitively a causal relationship between periodontitis in pregnancy and adverse pregnancy outcomes. The only definitive conclusion that can be reached is that there is a lot of evidence that women who have had adverse pregnancy outcomes have more of a tendency to have periodontitis than those who do not.
Introduction
The topic of the posited relationship between periodontal disease (periodontitis) in pregnant women and adverse pregnancy outcomes (premature labor, pre-term deliveries, small-for-gestational age infants, early or late miscarriages, low birth weights and eclampsia or preeclampsia) has received a lot of attention among researchers. During the last decade numerous investigators1-67 have reported or commented on the results of studies focusing on the topic. The majority of the empirical studies (at least twenty-three [3-4, 10, 15, 19, 22, 26, 28-29, 34, 36-38, 40, 43, 47-48, 56, 58, 62, 64-65, 67]), which include a range of methodological approaches and interventions, from prospective case-control studies to retrospective, non case-control studies using convenience samples, demonstrate to one degree or another a positive association between the presence of periodontal disease in pregnant mothers and diverse adverse pregnancy outcomes. This paper is devoted to a comprehensive literature review of the articles pertaining to this topic.
Methodology for Literature Review
Studies analyzed for inclusion in this literature review were identified from various sources: (1) Personal files of the authors. (2) References listed by previous investigators in their published articles. (3) Articles shared among colleagues. (4) Articles listed through PubMed©, a service of the National Library of Medicine and the National Institutes of Health. Copies of many of the articles were obtained through an interlibrary loan service of the University of Utah, Eccles Health Sciences Library, Salt Lake City, Utah.
The current authors read and examined the articles with the objectives of determining their contents in order to categorize them, i.e., empirical vs. non-empirical, positive associations, no associations, mixed results, summaries of previous studies; and to summarize the key findings and significance of disclosed associations. The current authors believe that the literature reviewed in this paper represents a relatively comprehensive list of studies pertaining to the topic as reported in the scientific literature over the last decade. No attempts were made to eliminate any particular periodicals except for those that may have been published in a foreign language for which English translations were locally unavailable. Table 1 is a numerical summary of the articles reviewed.
Results
This section delineates the results of the literature review. Literature is summarized in three categorical areas derived from the review process: (1) Studies Reporting Positive Associations; (2) Studies Reporting No Associations; (3) Studies Reporting Mixed or Equivocal Findings or Summaries of Previous Research Findings.
Studies Reporting Positive Associations
Possibly the first evidence of a positive relationship was reported in 1996 by Offenbacher, et al.[67] A case-control study of 124 pregnant or postpartum mothers, divided into case (preterm low birth weight or PLBW ) and control (normal birth weight or NBW) groups, disclosed worse periodontal disease among the former than the latter. The authors concluded that periodontal disease is a statistically significant risk factor for PLBW.
Other studies were reported in 1998. Davenport, et al.,[65] examined the relationship between maternal periodontal disease and PLBW. In their case-control study of 177 subjects, it was found that the extent and severity of periodontal disease were higher than predicted and may have reflected elevations in gingival inflammation associated with pregnancy.
Dasanayake,[62] in a 1:1 matched case-control study of 55 pairs of pregnant women, in which control variables were introduced, found that mothers of LBW infants were shorter, less educated, married to men of lower occupational status, had less healthy areas of gingival and more areas with bleeding and calculus, and gained less weight during pregnancy. The author concluded that poor periodontal health of the mother is a potential risk factor for LBW.
In another study of 1,313 pregnant women, Jeffcoat, et al.,[58] found that the data showed an association between the presence of periodontal disease at 24 weeks’ gestation and subsequent preterm birth.
In 2001, Offenbacher, et al.,[56] again reported on another five-year prospective study of 814 pregnant women. Their aim was to determine whether maternal periodontitis contributed to the risk for prematurity and growth restriction in the presence of traditional obstetric risk facts. The investigators concluded that the study provided evidence that periodontitis and incident progression are significant contributors to obstetric risk for preterm delivery, low birth weight and low weight for gestational age.
Lopez, et al.,48 conducted a randomized controlled study of 400 Chilean pregnant women with periodontal disease, randomly assigning 200 to an experimental group and 200 to a control group. They found that the incidence of PLBW in the treatment group was 1.8% and in the control group was 10.1%. In fact, periodontal disease was the strongest factor related to PLBW. Other factors significantly associated with PLBW were less than six pre-natal visits and maternal low weight gain.
In 2002, Riche, et al.,[47] reported on their study of 1,020 women, 47 of whom had preeclampsia. They found a strong association between periodontal disease status at enrollment and rate of premature delivery observed among preeclamptic women after adjusting for major risk factors, including maternal race, age, marital status, and use of WIC (women, infants’, children’s’ program) or food stamp services.
To determine if maternal periodontal disease is associated with the development of preeclampsia, Boggess, et al.,[40] studied 1,115 healthy pregnant women. After adjusting for other risk factors, they observed that active maternal periodontal disease during pregnancy is associated with an increased risk for the development of preeclampsia.
In the ensuing years, other studies have followed. Jeffcoat, et al.,[38] conducted a pilot study of 366 women, randomized to one of three treatment groups, and compared with an untreated reference group of 723 pregnant women. They noted that performing scaling and root planing in pregnant women may reduce preterm birth.
Radnai, et al.,[36] conducted a case-control study of postpartum women, 41 in a case group and 44 in a control group. A significant association was found between preterm birth and early localized peridontitis of patients.
A study by Goepfert, et al.,[34] of a convenience sample of 59 women who experienced a spontaneous preterm birth (SPB) at <32 weeks gestation, versus a control group of 36 women who experienced an indicated preterm birth at <32 weeks gestation, versus 44 women who experienced an uncomplicated term birth (TB) was revealing. The SPB group had significantly more extensive periodontitis that the TB group. Moreover, after controlling for maternal age, race, education, insurance status, parity, history of a SPB and smoking, women with severe periodontitis were almost three times as likely to experience a SPB as those without severe periodontitis.
In 2005, Marin, et al.,[26] reported on a study of 152 pregnant women, divided into three groups: healthy, gingivitis and periodontitis. They concluded that periodontal disease in normal Caucasian pregnant women, older than 25 years, is statistically associated with a reduction in infant birth weight.
Another study by Moliterno, et al.,[22] of 151 mothers, 76 in a case group and 75 in a control group, relying upon data from hospital registration records, indicated that periodontitis was a risk factor for low birth weight, similar to other risk factors already recognized by obstetricians.
Coming on the research scene again, Lopez, et al.,[19] reported the results of a randomized control trial of 870 pregnant women from Santiago, Chile. A treatment group of 580 women received periodontal treatment before 28 weeks gestation. A control group of 290 women received periodontal treatment after delivery. The treatment group had significantly reduced PTLBW.
More recently in 2006, Sadatmansouri, et al.,[10] reported the results of clinical trial research of 30 pregnant women (18-35 years of age) with moderate to severe periodontitis, 15 of which receive periodontal treatments and 15 of which did not receive treatments. The authors concluded that periodontal therapy results in a reduction in the PLBW rate.
Results of a prospective study were published by Offenbacher, et al.[4] They studied 1,020 pregnant women who received antepartum and postpartum periodontal examinations. It was found that maternal periodontal disease increased relative risk for preterm or spontaneous preterm births. In fact, periodontal disease progression during pregnancy was found to be a predictor of more severe adverse pregnancy outcome of very preterm birth, independent of traditional obstetric, periodontal and social domain risk factors.
Boggess, et al.,[3] also studied prospectively 1,017 women, risk ratio adjusted for age, smoking, drugs, marital and insurance status and preeclampsia. Their conclusion was that moderate or severe periodontal disease in early pregnancy is associated with delivery of a small-for-gestation-age infant.
Studies Reporting No Associations
At least five [6,21,23,35,42] of the empirical studies reported disclose no evidence of relationships between periodontal disease in pregnant women and adverse pregnancy outcomes.
Davenport, et al.,[42] reported in 2002 the results of a case-control study of 236 pregnant women cases and a daily random sample of 507 controls. They found no evidence for an association between PLBW and periodontal disease. They concluded that the results do not support a specific drive to improve periodontal health of pregnant women as a means of improving pregnancy outcomes.
In 2004, Moore, et al.,[35] completed and reported a prospective study of 3,738 women. They found no significant relationships between the severity of periodontal disease and either preterm or LBW. They observed, however, that there did “appear” to be a correlation between poorer periodontal health and those that experienced a late miscarriage. The major conclusion of the study was that there was no association between either preterm birth or LBW and periodontal disease in the study population.
A study was also conducted by Noack, et al.,[23] and reported in 2005. Of 59 pregnant women with a high risk of LBW (suffering from preterm contractions) versus 42 women with no preterm contractions and infants appropriate for date and weight, there were no significant differences between the groups in any aspects of the studied periodontitis parameters. Periodontitis was not noted to be a detectable risk factor for PLBW in pregnant women.
Also reported in 2005 was a study by Lunardelli and Peres.21 They tested the potential link between periodontal disease in pregnant women and LBW or prematurity. Relying on a population-based, cross-sectional study of 449 parturients in Southern Brazil, they found no association between the variables.
Michalowicz, et al.,[6] sought to study the effect of nonsurgical periodontal treatment on preterm birth. Their 2006 reported study of 823 women included random assignment of 413 patients to a treatment group which received scaling and root planning, compared to 410 patients in a control group which received no treatment. The authors concluded that treatment of periodontitis improves periodontal health and is safe, but does not significantly alter the rates of preterm birth, LBW or fetal growth restriction.
Studies Reporting Mixed or Equivocal Findings or Summaries of Previous Research Findings
The remainder of the published articles we analyzed, [1-2, 5, 7-9, 11-14, 16-18, 20, 24-25, 27, 30-33, 39, 41, 44-46, 49, 50-53, 55, 57, 59, 60-61, 63] both empirical and nonempirical reveal mixed findings, focus in a preliminary sense on the study of the role of antigens or pathogens in explaining the relationship, or provide summary commentary (from other literature reviews) about conclusions derived from studies already conducted. For example, Farrell, et al.,[11] reported mixed findings in their prospective study of 1,793 women reported never previously smoking. There was, in fact, an association between some measures of periodontal disease and late miscarriage, but no association between periodontitis and preterm birth or LBW in the study population.
In an earlier study Moreu, et al.,[24] based on examinations of 96 pregnant women in first, second and third trimester of pregnancy, observed mixed findings. They reported that periodontal disease is a significant risk factor for LBW but not for pre-term delivery.
Buduneli, et al.,[27] evaluated the possible link between periodontal infections and PLBW for post-partum women with low socioeconomic characteristics. They found no statistically significant differences between the cases and the controls regarding dental and periodontal parameters. Bacterial load scores, however, were significantly higher in the controls than in the cases.
Similarly, but conversely, Mitchell-Lewis, et al.,[53] in a study of 213 pregnant women, with 74 assigned to a treatment group and 90 to a non treatment group, found mixed results. They observed no differences in clinical periodontal status between the two groups. However, PLBW mothers had significantly higher levels of certain bacteria.
Some studies are beginning to identify potential pathogens (organisms) and the potential roles they may play in fostering the relationship. Hill (1998),[66] examined the effects of a complex of bacterial vaginosis microbes and their impact of PLBW. The study provided evidence associating maternal periodontal disease with PLBW taken with the isolation of F. nucleatum, Capnocytophaga, and other oral species from amniotic fluid.
Dasanayake, et al.,[52] studied 448 women, predominantly African American and socioeconomically homogeneous, using case and control groups. Their data showed that LBW deliveries were associated with a higher maternal serum antibody level against P. gingivalis at mid-trimester. The association remained significant after controlling for smoking, age lgG levels against other selected periodontal pathogens, and race.
One analytical study in 2001 by Madianos, et al.,[55] of 812 deliveries from a cohort study of pregnant mothers presented measures of maternal periodontal infection using whole chromosomal DNA probes to identify 15 periodontal organisms within maternal periodontal plaque sampled at delivery. A conclusion was proffered: the high prevalence of elevated fetal lgM to C. rectus among premature infants raises the possibility that this specific maternal oral pathogen may serve as a primary fetal infectious agent eliciting prematurity.
A study reported in 2006 by Yiping, et al.,[9] of 34 pregnant women also provided some direct evidence of oral-utero microbial transmission. The authors stated that their observations suggested a Bergeyella strain identified in the patient’s intrauterine infection originated from the oral cavity.
Some of the reported studies mentioned previously have engendered commentary about the reliability and validity of the investigations, some of it controversial about whether some of the results from different studies are in conflict, or and about the need for more skillful appraisals of the methodologies used in the analyses. One commentator, Ahearne,[31] suggested that “the concept of evidence based dentistry is an honorable one, but the reality is that it can become very confusing for the practicing dentist when different studies ask the same question but come up with different answers.” Ahearne first referred to the study by Moore, et al.,[35] in which no positive relationship was found between periodontal disease and pre-term birth or LBW. Secondly, he noted that the very same month Radnai, et al.,[36] asked a very similar question and came to the conclusion that peridontitis was an important risk factor for pre-term birth. The conclusion of the letter was that “if the difference in the outcomes of the studies is due to the difference in the populations studied then, surely it raises some questions about the validity of clinical trials in general.”
In a follow-up research letter, Beckett, et al.,[25] using “a systematic process of critical appraisal, discovered that one of the studies contained a far more reliable evidence source than the other.” They recommended that “practitioners must develop critical appraisal skills. It is important not to fall into the trap of assuming because a paper is published in a referred journal, it must be sound. . . .”
One interesting study contained an insightful meta analysis of previous research. Khader and Ta’ani,[29] in a methodologically sophisticated review of previous studies, utilizing independently abstracted data from the studies, found that periodontal diseases in the pregnant mother significantly increases the risk of subsequent prê-term birth or LBW. Their conclusion was based on two previous case-control studies and three prospective cohort studies that met prestated meta analysis inclusion criteria. Another interesting conclusion was reached: “there is no convincing evidence, on the basis of existing case-control and prospective studies, that treatment of periodontal disease will reduce the risk of pre-term birth.”
Conclusions
The majority of reported studies indicate a positive association between periodontitis in pregnant mothers and adverse pregnancy outcomes. Although a plethora of research has already occurred, clearly there still isn’t sufficient evidence, however, to conclude a causal relationship between the presence of periodontitis and adverse pregnancy outcomes. The only definitive conclusion that can be reached is that there is a lot of evidence of a positive association of periodontitis with adverse pregnancy outcomes. In other words, those women who have had adverse pregnancy outcomes have more of a tendency to have periodontitis than those who do not. This fact is evident even when various control variables are analyzed as potential explanations or reasons for the relationship. The precise mechanisms or chemical processes that would establish a definitive causal relationship have not yet been unequivocally identified. Further research to identify and isolate causal mechanisms or processes still needs to be undertaken. It would be wise to conduct a prospective case-control study in which an adequate sample of subjects is included, and multiple regression is applied to assess the independent contributions (amount of variance accounted for) of various variables that are known to predispose to adverse pregnancy outcomes.
Despite the lack of conclusive causal explanations, proper prophylaxes should still be encouraged. There isn’t any evidence to suggest that proper prophylaxes won’t be beneficial to pregnant women, and it is likely more prudent to err on the side of prevention rather than doing nothing.
References
- Bobetsis, Y.A., Barros, S.P., & Offenbacher, S. (2006). Exploring the relationship between periodontal disease and pregnancy complications. J Am Dent Assoc 137 (Suppl. 2), 7S-13S.
- Douglass, C.W. (2006). Risk assessment and management of periodontal disease. J Am Dent Assoc 137 (Suppl. 3), 27S-32S.
- Boggess, K.A., Beck, J.D., Murtha, A.P., Moss, K. & Offenbacher, S. (2006). Maternal periodontal disease in early pregnancy and risk for a small-for-gestational-age infant. Am J Obstet & Gynecol 194, 1316-22.
- Offenbacher, S., Boggess, K.A., Murtha, A.P., Jared, H.L., Lieff, S., McKaig, R.G., Mauriello, S.M., Moss, K.L., & Beck, J.D. (2006). Progressive periodontal disease and risk of very preterm delivery. Am J Obstet & Gynecol 107, 29-36.
- Goldenberg, R.L., & Culhane, J.F. (2006, Nov.). Preterm birth and periodontal disease. N Engl J Med 355(18), 1925-27.
- Michalowicz, B.S., Hodges, J.S., DiAngelis, A.J., Lupo, V.R., Novak, M.J., Ferguson, J.E., Buchanan, W., Bofill, J., Papapanou, P.N., Mitchell, D.A., Matseoane, S., & Tschidi, P.A. (2006, Nov.). Treatment of periodontal disease and the risk of preterm birth. N Eng J Med 355(18), 1885-94.
- Goldie, M.P. (2006, Aug.). Healthy mother, healthy baby. Int J Dent Hyg 67(6), 162-3.
- Nesse, W., Spijkervat, F.K., Abbis, F., & Vissink, A. (2006, May). Links between periodontal disease and general health. 2. Preterm birth, diabetes and autoimmune diseases. Ned Tijdschr Tandheelkd 113(5), 191-6.
- Yiping, H., Ikegami, A., Bissada, N., Herbst, M., Redline, R., & Ashmead, G.G. (2006, Apr.). Transmission of an uncultivated bergeyella strain from the oral cavity to the amniotic fluid in a case of preterm birth. J Clin Microbiology 44(4), 1475-83.
- Sadatmansouri, S., Sedighpoor, N., & Aghaloo, M. (2006, Mar.). Effects of periodontal treatment phase I on birth term and birth weight. J Indian Soc Pedod Prev Dent 24(1), 23-6.
- Farrell, S., Ide, M., & Wilson, R.F., (2006, Feb.). The relationship between maternal periodontitis, adverse pregnancy outcome and miscarriage in never smokers. J. Clin Peridontol 33(2), 115-20.
- Vettore, M.V., Sheiham, A., & Peres, M.A. (2006, Feb.). Low birth weight and periodontal diseases association. Rev Saude Publica 40(1), 184-5, 181-2, author reply 185-6, 182-3.
- Xiong, X., Buekens, P., Vastardis, S., & Wu, T. (2006). Periodontal disease as one possible explanation for the Mexican paradox. Med Hypoth 67(6), 1348-54.
- Xiong, X., Buikens, P., Fraser, W.D., Beck, J., & Offenbacher, S. (2006, Feb.). Periodontal disease and adverse pregnancy outcomes: a systematic review. Brit J Obstet & Gynecol 113(2), 135-43.
- Urban, E., Radnai, M., Novak, T., Gorzio, I., Pal, A., & Nagy, E. (2006, Feb.). Distribution of anaerobic bacteria among pregnant periodontitis patients who experience preterm delivery. Anaerobe 12(1), 52-7.
- Rajapakse, P.S., Nagarathne, M., Chandrasekra, K.B., & Dasanayake, A.P. (2005). Periodontal disease and prematurity among non-smoking sri lankan women. J Dent Res 84(3), 274-77.
- Editor. (2005, Dec.). Periodontal therapy and pregnancy. Br Dent J 199(11), 697.
- Mealey, B.L., & Moritz, A.J. (2005, Dec.). Pregnancy and the periodontium. Tex Dent J 122(12), 1204-11.
- Lopez, N.J., Da Silva, I., Ipinza, J., & Gutierrez, J. (2005, Nov.). Periodontal therapy reduces the rate of preterm low birth weight in women with pregnancy-associated gingivitis. J Periodontol 76(11 Suppl.), 886-90.
- Qureshi, A., Ijaz, S., Syed, A., Quershi, A., & Khan, A.A. (2005, Oct.). Periodontal infection: a potential risk factor for preterm delivery of low birth weight (PLBW) babies. J Pak Med Assoc 55(10), 448-52.
- Lunardelli, A.N. & Peres, M.A. (2005, Sep.). Is there an association between periodontal disease, prematurity and low birth weight? A population-based study. J Clin Periodontol 32(9), 938-46.
- Moliterno, L.F., Monteiro, B., Figueredo, C.M., & Fischer, R.G. (2005, Aug.). Association between periodontitis and low birth weight: a case-control study. J Clin Peridontol 32(8), 886-90.
- Noack, B., Klingenberg, J., Weigelt, J., & Hoffman, T. (2005, Aug.). Periodontal status and preterm low birth weight: a case control study. J Periodontal Res 40(4), 339-45.
- Moreu, G., Tellez, L., & Gonzalez-Jaranay, M. (2005, June). Relationship between maternal periodontal disease and lowbirth- weight pre-term infants. J Clin Periodontol 32(6), 622-27.
- Beckett, H., Ramsey, R., Thompson, B., & Brennan, P.A. (2005, May). Journal clubs. Br Dent J 198(10), 629.
- Marin, C., Segura-Egea, J.J., Martinez-Sahuquillo, A., & Bullon, P. (2005, Mar.) Correlation between infant birth weight and mother’s periodontal status. J Clin Periodontol 32(3), 299-304.
- Buduneli, N., Baylas, H., Buduneli, E., Turkoglu, O., Kose, T., & Dahlen, G. (2005, Feb.). Periodontal infections and pre-term low birth weight: a case-control study. J Clin Periodontol 32(2), 174-81.
- Jarjoura, K., Devine, P.C., Perez-Delboy, A., Herrera-Abreu, M., D’Alton, M., & Papapanou, P.N. (2005, Feb.). Markers of periodontal infection and preterm birth. Am J Obstet & Gynecol 192(2), 513-9.
- Khader, Y.S. & Quteish, T. (2005, Feb.). Periodontal diseases and the risk of preterm birth and low birth weight: a meta-analysis. J Periodontol 76(2), 161-65.
- Yeo, B.K., Lim, L.P., Paquette, D.W., & Williams, R.C. (2005, Jan.). Periodontal disease—the emergence of a risk for systemic conditions: pre-term low birth weight. Ann Acad Med Singapore 34(1), 111-6.
- Ahearne, J. (2004, Nov.). Evidence based dentistry. Br Dent J 197(10), 594.
- Bonett, J.B. (2004, Fall). Exploring the link. Periodontitis and preterm birth. Penn Dent J 2004, Fall, 10-3.
- Konopka, T. (2004, May). Periodontitis and preterm low birth weight. Ginekol Pol 75(5), 397-403.
- Goepfert, A.R., Jeffcoat, M.K., Andrews, W.W., et al. (2004, Oct.). Periodontal disease and upper genital tract inflammation in early spontaneous preterm birth. Am J Obstet & Gynecol 104(4), 777-83.
- Moore, S, Ide, M., Coward, P.Y., Randhawa, M., Borkowska, E., Baylis, R., & Wilson, R.F. (2004, Sep.). A prospective study to investigate the relationship between periodontal disease and adverse pregnancy outcome. Br Dent J 197(5), 251-58.
- Radnai, M., Gorzo, I., Nagy, E., Urban, E., Novak, T., & Pal, A. (2004, Sep.). A possible association between preterm birth and early periodontitis: a pilot study. J Clin Periodontol 31(9), 736-41.
- Hasegawa, K., Furuichi, Y., Shimotsu, A., Hakamura, M., Yoshinaga, M., & Kamitomo, M. (2003, Dec.). Associations between systemic status, periodontal status, serum cytokine levels, and delivery outcomes in pregnant women with a diagnosis of threatened premature labor. J Periodontol 74(12), 1764-70.
- Jeffcoat, M.K., Hauth, J.C., Geurs, N.C., Reddy, M.S., Cliver, S.P., Hodgkins, P.M., & Goldenberg, R.L. (2003, Aug.). Periodontal disease and preterm birth: results of a pilot intervention study. J Periodontol 74(8), 1214-18.
- Kadowski, T., Takii, R., Baba, A., & Yamamoto, K. (2003, July). Gingipains as the determinants of periodontopathogenicity. Nippon Yakurigaku Zasshi 122(1), 37-44.
- Boggess, K.A., Lieff, S., Murtha, A.P., Moss, K., Beck, J., & Offenbacher, S. (2003, Feb.) Maternal periodontal disease is associated with an increased risk of preeclampsia. Am J Obstet & Gynecol 101(2), 227-31.
- Bearfield, C., Davenport, E.S., Sivapathasundaram, V., & Allaker, R.P. (2002, May). Possible association between amniotic fluid micro-organism infection and microflora in the mouth. Brit J Ob Gyn 109(5), 527-33.
- Davenport, E.S., Williams, C., Sterne, J., Murad, S., Sivapathasundram, V., & Curtis, M.A. (2002). Maternal periodontal disease and preterm low birthweight: case-control study. J Dent Res 81(5), 313-18.
- Lopez, N.J., Smith, P.C., & Gutierrez, J. (2002). Higher risk of preterm birth and low birth weight in women with periodontal disease. J Dent Res 81(1), 58-63.
- Otomo-Corgel, J., & Merin, R.L. (2002, Apr.). Periodontol disease and systemic health–what you and your patients need to know. J Calif Dent Assoc 30(4), 307-11.
- Rose, L.F., Steinberg, B.J., & Minsk, L. (2002). Periodontal disease and systemic disease. Clinical information for the practicing dentist. J Indiana Dent Assoc 81, 15-18.
- Radnai, M., & Gorzo, I. (2002, Dec.). Periodontal disease as a potential risk factor for preterm birth and low birth weight (literature review). Fogorv Sz 95(6), 241-44. (Article in Hungarian).
- Riche, E.L., Boggess, K.A., Lieff, S., Murtha, A.P., Auten, R.L., Beck, J.S., & Offenbacher, S. (2002, Dec.). Periodontal disease increases the risk of preterm delivery among preeclamptic women. Ann Periodontol 7(1), 95-101.
- Lopez, H.J., Smith, P.C., & Gutierrez, J. (2002, Aug.). Periodontal therapy may reduce the risk of preterm low birth weight in women with periodontal disease: a randomized controlled trial. J Periodontol 73(8), 911-24.
- Krejci, C.B., & Bissada, N.F. (2002, Mar.). Women’s health issues and their relationship to periodontitis. J Am Dent Assoc 133(3), 323-9.
- McGaw, T. (2002, Mar.). Periodontal disease and preterm delivery of low-birth-weight infants. J Can Dent Assoc 68(3), 165-9.
- Teng, Y.T., Taylor, G.W., Scannapieco, F., Kinane, D.F., Curtis, M., Beck, J.D., & Kogon, S. (2002, Mar.). Periodontol health and systemic disorders. J Can Dent Assoc 68, 188-92.
- Dasanayake, A.,P., Boyd, D., Madianos, P.N., Offenbacher, S., & Hills, E. (2001, Nov.). The association between porphyromonas gingivalis-specific maternal serum lgG and low birth weight. J Periodontol 72(11), 1491-97.
- Mitchell-Lewis, D., Engebretson, S.P., Chen, J., Lamster, I.B., & Papapanou, P.N. (2001). Periodontal infections and pre-term birth: early findings from a cohort of young minority women in New York. Eur J Oral Sci 109, 34-39.
- Slots, J, & Kamma, J.J. (2001). General health risk of periodontal disease. Intern Dent J 51(5), 417-27.
- Madianos, P.N., Lieff, S., Murtha, A.P., Boggess, K.A., Auten Jr., R.L., Beck, J.E., & Offenbacher, S. (2001, Dec.). Maternal periodontitis and prematurity. Part II: maternal infection and fetal exposure. Ann Periodontol 6(1): 175-82.
- Offenbacher, S., Lieff, S., Boggess, K.A., Murtha, A.P., Madianos, P.N., Champagne, C.M.E., McKaig, R.G., Jared, H.L., Mauriello, S.M., Auten Jr., R.L., Herbert, W.N.P., & Beck, J.D. (2001, Dec.). Maternal periodontitis and prematurity. Part I: obstetric outcome of prematurity and growth restriction. Ann Periodontol 6(1), 164-74.
- Jeffcoat, M.K., Geurs, N.C., Reddy, M.S., Goldenberg, R.L., & Hauth, J.C. (2001, Dec.). Current evidence regarding periodontal disease as a risk factor in preterm birth. Ann Periodontol 6(1), 183-88.
- Jeffcoat, M.J., Geurs, N.C., Reddy, M.S., Cliver, B.S., Goldenberg, R.L., & Hauth, J.C., (2001, July). Periodontal infection and preterm birth results of a prospective study. J Am Dent Assoc 132, 875-88.
- Leone, C.R. (2001, Jan-Feb). Maternal periodontal disease and premature birth or low birth weight. J Pediatr (Rio J) 77(1), 6-7.
- Engebretson, S.P., Lalla, E., & Lamster, I.B. (1999, Oct.). Periodontitis and systemic disease. N Y State Dent J 65(8), 30-2.
- Goldenberg, R.L., Rouse, D.J. (1998, July). Prevention of premature birth. N Engl J Med 339(5), 313-20.
- Dasanayake, A.P. (1998, July). Poor periodontal health of the pregnant woman as a risk factor for low birth weight. Ann Periodontol 3(1), 206-12.
- Offenbacher, S., Jared, H.L., O’Reilly, P.G., et al (1998, July). Potential pathogenic mechanisms of periodontitis-associated pregnancy complications. Ann Periodontol 3(1), 233-50.
- Offenbacher, S., Beck, J.D., Lieff, S., & Slade, G. (1998, Oct.). Role of periodontitis in system health: spontaneous preterm birth. J Dent Educ 62(10), 852-8.
- Davenport, E.S., Williams, C.E., Sterne, J.A., Sivapathasundram, V., Fearne, J.M., & Curtis, M.A. (1998, July). The east London study of maternal chronic periodontal disease and preterm low birth weight infants: study design and prevalence data. Ann Periodontol 3(1), 213-21.
- Hill, G.B. (1998, July). Preterm birth: associations with genital and possibly oral microflora. Ann Periodontol 3(1), 222-32.
- Offenbacher, S., Katz, V., Fertik, G., Collins, J., Boyd, D., Maynor, G., McKaig, R. & Beck, J. (1996, Oct.). Periodontal infection as a possible risk factor for preterm low birth weight. J Periodontol 67(Suppl.), 1103-13.
